
Editor's note, April 2026. The framework introduced in this series under the name Constraint Failure Model (CFM) is now called the Signal Loss Model (SLM). The three mechanisms have been renamed: SCT → Untethered Cognition (UC), IH → Neuroimmune Dysregulation (ND), RDIS → Pursuit-Reward Decoupling (PRD). The underlying logic is unchanged. For the full rationale, see On Renaming: From Constraint Failure to Signal Loss. The essays below retain their original titles and are being revised in place.
The Essays
SLM1—Why Your Depression Might Not Be a Disease
Uses recent Nature-published genetic and metabolic research to show that depression, anxiety, and PTSD are not discrete diseases, but symptom clusters emerging from shared biological substrates—forcing a rethink of the biomedical model itself.
Explains how human cortical expansion, combined with the removal of real-world constraint, causes internal simulation to decouple from reality—producing rumination, anxiety, and cognitive instability.
Shows why the same underlying architecture collapses differently in high achievers, burned-out strivers, and post-achievement individuals, depending on how constraint is applied or removed across the lifespan.
SLM4—Inflammation as Lock-In, Not Side Effect
Details how chronic stress drives an inflammatory cascade that suppresses neuroplasticity, biologically freezing maladaptive patterns and explaining why insight alone often fails.
SLM5—When Nothing Feels Worth Doing
Describes how sustained cortisol elevation downregulates dopamine receptors, collapsing incentive salience and motivation—and why “trying harder” cannot restore it.
Integrates untethered cognition, neuroimmune dysregulation, and pursuit-reward decoupling into a single self-reinforcing system that explains the persistence and treatment resistance of modern psychological distress.
SLM7—Choosing Interventions Without Magical Thinking
Introduces an epistemological framework for intervention selection, clarifying why some (otherwise sensible) approaches fail because they are applied at the wrong biological moment.
This addendum supplements SLM7 Section III (”Biological State First”) and the discussion of neuroplasticity availability. It does not alter the essay’s argument. It strengthens one leg of it (the inflammaging cascade) with evidence that arrived too late for the original draft and too early to ignore.
SLM8—Psychedelics as Windows, Not Solutions
Explains why psychedelics reliably open temporary plasticity windows by resetting autonomic balance, while emphasizing why disruption alone rarely produces durable change.
SLM9—Constraint Installation During Plasticity Windows
Shows how precisely timed, embodied, and relational constraints can recalibrate simulation machinery and reward systems while the brain is biologically capable of rewiring.
Examines the clinical trial relapse data as a dataset, explains why plasticity windows are actively closed by dedicated biological machinery, and argues that the field’s current model of integration fails because it operates at the wrong level of mechanism.
Nāhua serves more than one kind of person—and more than one kind of problem.
Some guests arrive carrying acute distress: depression, anxiety, trauma, grief. Others arrive functional on the surface but profoundly disoriented beneath it—successful, capable, and stuck in ways that standard explanations fail to capture.
The Signal LossModel (SLM) exists for the latter group.
This index introduces a limited 10-part scientific series exploring the model that explains a specific, predictable form of psychological collapse seen most often in high-functioning, post-achievement, or chronically overextended individuals. It is not a universal theory of mental illness, and it is not the sole rationale for Nāhua. It is one operating system within a broader therapeutic architecture.
What SLM Is and Is Not
SLM is a mechanistic model, not a diagnosis.
It explains how certain minds fail because the environments that once constrained and organized them have either disappeared or become unsustainable. These are not “weak” or “broken” minds.
Specifically, SLM addresses what Nāhua internally refers to as the Achievement Paradox transition: the moment when the cognitive machinery that once produced success begins producing suffering instead.
SLM does not attempt to explain:
Primary trauma disorders (PTSD)
Typical Major Depressive Disorder (MDD)
Generalized Anxiety Disorder (GAD)
Severe psychiatric pathology
Many Nāhua guests fall outside the SLM profile—and are supported using different models, sequences, and emphases.
The Model, Defined
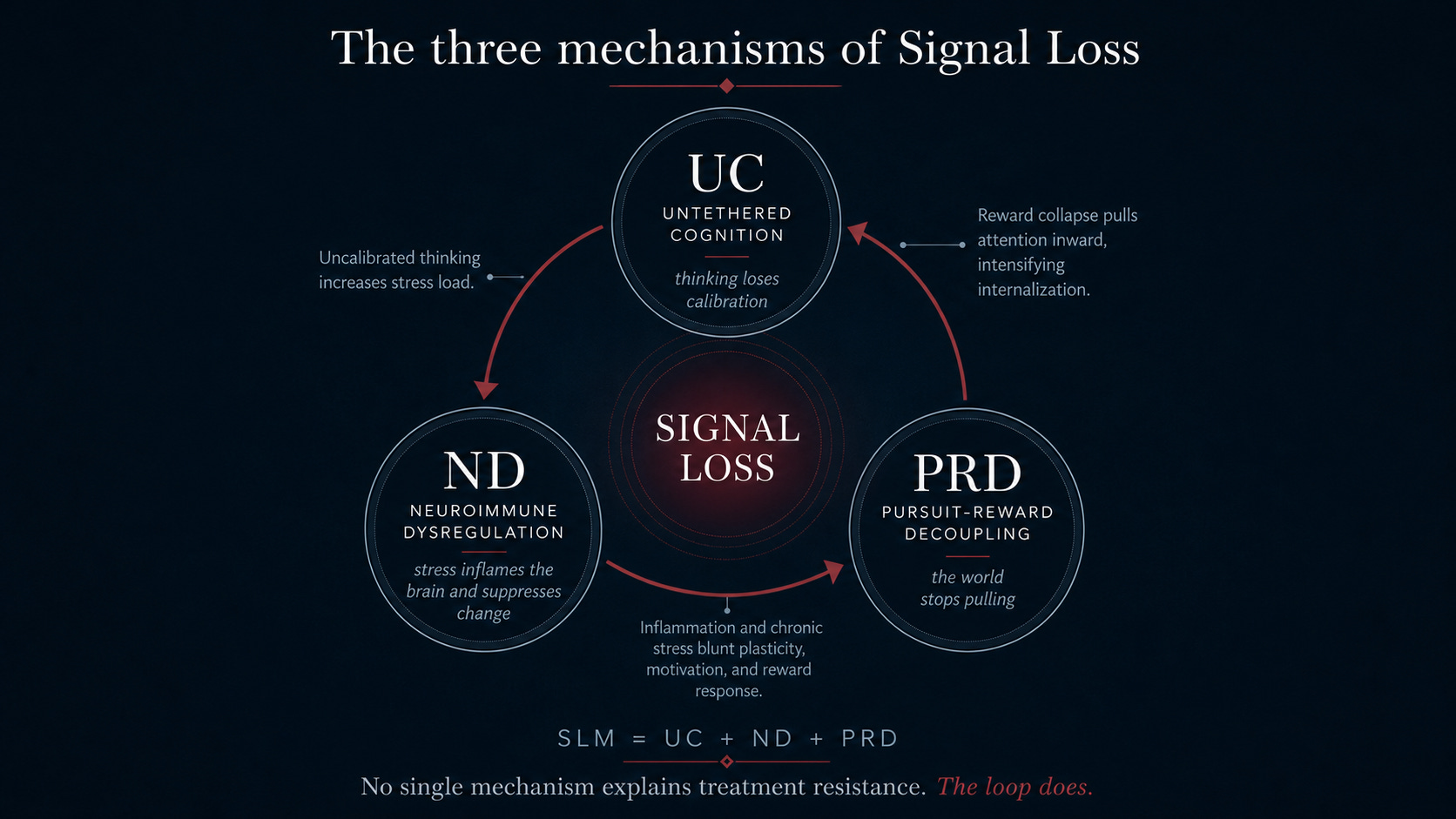
The Signal Loss Model is not a single theory. It is the emergent intersection of three well-defined mechanisms, each insufficient on its own, but explanatory in combination.
SLM = UC + ND + PRD
1. Untethered Cognition (UC)
A cognitive-architectural account of how advanced human cognition , often referred to as “simulation” in the scientific literature (planning, abstraction, narrative identity), depends on continuous real-world calibration—and what happens when that constraint is lifted or becomes pathological.
2. Neuroimmune Dysregulation (ND)
A biological account of how chronic stress, unresolvable threat modeling, and autonomic imbalance produce persistent low-grade inflammation that suppresses neuroplasticity and locks maladaptive patterns in place.
3. Pursuit-Reward Decoupling (PRD)
A motivational account of how sustained cortisol elevation downregulates dopamine signaling, causing the external world to lose motivational pull—driving the mind further inward and reinforcing the collapse.
Together, these three mechanisms describe a self-reinforcing system failure:
uncalibrated thinking → chronic stress → inflammation → reward collapse → further internalization.
SLM names that loop, explains why it is stable, and clarifies why many otherwise effective interventions fail when applied in the wrong biological window or environmental context.
Why This Series Exists
This series is not required reading to attend Nāhua.
It exists for three reasons:
For guests who recognize themselves in this pattern and want a rigorous explanation for why insight alone hasn’t been enough.
For clinicians and scientists evaluating Nāhua’s protocol design and theoretical grounding.
For readers interested in the architecture of modern psychological collapse, particularly among high-functioning populations.
Each essay builds on the last. The series is cumulative by design and best read in order.